Fallopian Tube Anatomy
What is tubal ligation?
 Tubal ligation is the general term for any surgical procedure that blocks the fallopian tubes to prevent pregnancy.
Tubal ligation is the general term for any surgical procedure that blocks the fallopian tubes to prevent pregnancy.
The fallopian tube is not just a tube…it is an intricate organ that helps with conception. The fallopian tube allows sperm to get to the egg and provides a supportive environment for fertilization. The fallopian tube perfectly times the transport of the fertilized, growing egg to the uterus so implantation can occur.
Sperm enter the fallopian tube through the uterus. The ovary releases the egg and the egg enter the fallopian tube from the ovarian or fimbrial end of the tube. When the fallopian tubes are blocked, sperm and eggs are kept apart and fertilization is prevented.
Ligation means to apply a ligature (suture) and tubal ligation is often called “tying” the tubes.
Many people picture tying a fallopian tube like tying a shoe lace or a bow, and wonder why the tube can’t simply be untied to restore fertility. To explain this, the anatomy of the normal fallopian tube is shown on this page.
Fallopian tube anatomy
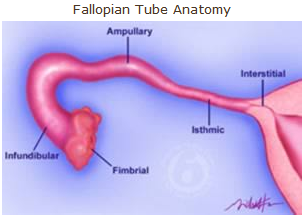 The fallopian tube is a narrow muscular organ arising from the uterus and ending just next to the ovary. The inner tubal lining is rich in cilia, the microscopic hair-like projections that beat in waves and move the egg to the uterus.
The fallopian tube is a narrow muscular organ arising from the uterus and ending just next to the ovary. The inner tubal lining is rich in cilia, the microscopic hair-like projections that beat in waves and move the egg to the uterus.
The cilia are what causes the fluid to flow towards the uterus and carry the fertilized egg to the uterus for implantation.
The fallopian tube is about 6 inches long and consists of several segments. Starting from the uterus and proceeding toward the ovary, these are:
- Interstitial segment — passes through the uterine muscle
- Isthmic segment — narrow muscular segment by the uterus
- Ampullary segment — wider middle segment
- Infundibular segment — funnel shaped segment near the ovary
- Fimbrial segment — ciliary lining facing the ovary
Fallopian tube anatomy: Where is the blockage?
The success of tubal reversal surgery often depends on the age of the patient at the time of reversal and the type of tubal ligation procedure. Tubal ligations that due more damage and shorten the tube decrease the chance of pregnancy.
The location of the tubal ligation on the fallopian tube is also helpful in predicting the success of tubal reversal.
The fallopian tube is like a funnel…it is narrow near the uterus and wide near the ovary. The fallopian tube is the narrowest where it inserts into the uterine muscle. The fallopian tube is the widest near the ovary.
Understanding fallopian tube anatomy and the location of the blockage will help you to better understand the chance of getting pregnant after tubal ligation reversal.
Interstitial fallopian tube blockage
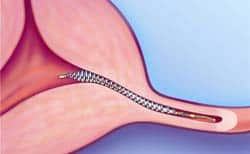 Interstitial fallopian tube blockage is most commonly caused by Essure and Adiana type tubal occlusion procedures.
Interstitial fallopian tube blockage is most commonly caused by Essure and Adiana type tubal occlusion procedures.
Noticed that we used the word ‘occlude’. Tubal occlusion is the medical term for causing the tube to be closed from the inside out…so rather then tying or clamping the tube from the outside to cause it to close… Essure or Adiana devices are inserted into the tube to cause the tube to close.
Occasionally coagulation (burning) type tubal ligations can also cause blockage in the interstitial area. On rare occasions previous pelvic infection or fibroid removal surgery can cause complete blockage of the interstitial portions of one or both fallopian tubes.
There is also a disease condition called Salpingitis Isthmica Nodosa. This causes inflammation and closure of the interstitial segment of the fallopian tubes.
Repair of tubal blockage in the interstitial fallopian tube is extremely challenging because this is the smallest portion of the tube. This area is technically more difficult to repair and there is a higher risk the tube can heal closed in the area of the repair within the first six (6) months of reversal surgery.
Reversal of interstitial blockage requires a tubouterine implantation procedure. This is where the blocked portion is removed and the remaining healthy fallopian tube is reinserted into a new opening created in the uterine muscle.
The chance of pregnancy after tubouterine implantation ranges from 40% to 60%.
Isthmic fallopian tube blockage
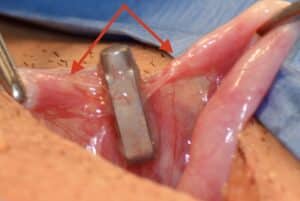 The isthmic section of the fallopian tube is wider than the interstitial section. Not only is the isthmic fallopian tube wider but it is also more muscular and thicker. The isthmic section is usually where tubal clips and tubal rings are placed.
The isthmic section of the fallopian tube is wider than the interstitial section. Not only is the isthmic fallopian tube wider but it is also more muscular and thicker. The isthmic section is usually where tubal clips and tubal rings are placed.
The isthmic section is probably the best area of the fallopian tube to have blockage.
When tubal clips (Filshie or Hulka) clips are placed in this area the chance of pregnancy success after repairing blockage caused by these devices can be as high as 80% to 90%.
There seems to be a lower chance of the tubes healing closed after repairs in the isthmic section of the fallopian tube.
Ampullary fallopian tube blockage
The ampullary portion of the fallopian tube is much wider than the isthmic section. As the tube gets wider, the muscular layer becomes thinner. The walls of the fallopian tube are thinner and rejoining these tubal walls can be more difficult.
The ampullary section of the fallopian tube is usually where tying and cutting and tubal burning procedures are performed.
The problem with tubal ligation procedures in this area of the tube….is not with the technique but rather the amount of tube that is damaged. Each doctor performs these procedures differently.
When a large section of the ampullary portion of the tube is cut out and removed….or burned…..then the remaining tubal segments can be very healthy but different in tubal diameters.
 The fallopian tube is not uniform in size like a garden hose.
The fallopian tube is not uniform in size like a garden hose.
Remember we said the fallopian tube is like a funnel that goes from very wide near the ovary (to help catch and egg) to very narrow as it goes into the muscle (to help funnel the egg into the uterine cavity faster for implantation).
When large sections of the ampullary portion of the fallopian tube are removed with cutting and tying or burning then that leaves two segments of the tube remaining: a segment near the ovary (ovarian) and a segment near the uterus (uterine).
The challenge with repairing this blockage is the ovarian segment is often much wider than the uterine segment.
The chance of pregnancy success after repair of these types of tubal ligations done in the ampullary portion is about 60%. These repairs can sometimes heal closed after surgery. We estimate the chance of tubal closure of repairs in this area are 10% to 15%.
Infundibular fallopian tube blockage
The infundibular section of the tube is a vague concept to understand. It is not the end of the tube but it is not the middle of the tube. The term is more of a historical anatomy term.
The problem with tubal ligations in the infundibular section of the tube is that the ovarian end of the remaining tube is short. It is either fimbrial tissue only or sometimes nothing at all.
When patients send us tubal ligation reports and their pathology report indicates 3 cm or more of tube have been removed we are sometimes concerned the tubal ligation may extend to the infundibular or fimbrial portion of the fallopian tube.
Fimbrial fallopian tube blockage
Blockage of the fimbrial end of the tube can occur from tying and cutting tubal ligation procedure or tubal burning procedures.
 It is becoming increasingly more common to remove the fimbrial end of the fallopian tube during tubal ligation procedures. This procedure is called a fimbriectomy tubal ligation. This is to completely remove the fimbrial end of the tube tube.
It is becoming increasingly more common to remove the fimbrial end of the fallopian tube during tubal ligation procedures. This procedure is called a fimbriectomy tubal ligation. This is to completely remove the fimbrial end of the tube tube.
Fimbrial tubal blockage can also occur from pelvic infections caused by chlamydia or gonnoreha…more commonly known as PID.
Fimbriectomy tubal ligation can be reversed with a procedure called a fimbriectomy reversal or ampullary salpingostomy. This procedure involves creating a new opening in the ampullary portion of the fallopian tube.
The chance of pregnancy after reversal of fimbriectomy type tubal ligation ranges from 15% to 40% but is probably closer t0 15% chance of pregnancy.
Ampullary salpingostomy can also be used to repair blockage from tubal closure from prior pelvic infection. As long as the infection did not cause severe scarring or scar tissue formation throughout the entire pelvis and as long as the rest of the fallopian tube is not extensively damaged, ie swollen into a tubal hydrosalpinx (tube swollen with fluid), then opening of this type of blockage could give a chance of pregnancy higher than 20%.
Tubal ligation procedures
The tubal ligation procedures described in the pages that follow are the:
- Pomeroy tubal ligation
- Tubal rings and clips
- Monopolar and bipolar tubal coagulation
- Parkland and Irving Procedures
- Essure and Adiana (Hysteroscopic tubal occlusion procedures)
More information: Types of tubal ligations and how they are reversed
Types of tubal ligations that can be reversed!
If you would like to learn more about the different types of tubal ligation than can be reversed then we encourage you to watch this video.
Most tubal ligation procedures can be reversed. If you would like to know if you are a candidate for tubal ligation reversal surgery then you can send your records to Dr. Monteith for a free review.
For more information on how to send your records visit: Sending records to A Personal Choice
Having reversal surgery with A Personal Choice is easy!
Having reversal surgery with A Personal Choice is easy. All you have to do is send your tubal ligation records (if available) for a free review.
You can call (919) 977-5050 and speak with a helpful staff person if you have questions.
Once they determine you are a candidate you can schedule over the phone and using email. You would then travel to Raleigh, North Carolina to have outpatient surgery.
 You would stay three (3) days and two (2) nights. Your consultation is on the first day, your surgery is on the second day, and your postoperative visit is on the third day.
You would stay three (3) days and two (2) nights. Your consultation is on the first day, your surgery is on the second day, and your postoperative visit is on the third day.
Surgery is in the outpatient surgery operating room which is located inside the A Personal Choice surgical facility.
Patients stay at a local hotel while having their surgery and they are required to bring a responsible adult with them over the age of 18 to help them the day of surgery and during their return home.
Patients travel from across the world to have surgery at A Personal Choice because of their excellence and dedication to offering affordable outpatient tubal reversal surgery.
