Tubal Ligation Pain
Can Endometrisosis Explain Some Cases?
As a practicing generalist, I frequently evaluated patients with acute and chronic pain because of endometriosis. Often this endometriosis was located in the anterior cul de sac (in front of the uterus) and posterior cul de sac (behind the uterus) and the ovary. I cannot recall diagnosing endometriosis involving the fallopian tube muscularis.
Subsequently, I began to exclusively perform tubal ligation reversal surgery and tubal repair surgery. I would often see women who complained of tubal ligation pain after sterilization. I frequently began to encounter pigmented endometriosis which exclusively involved the fallopian tubes and broad ligaments in the area where the tubal ligation was performed. Often these patients would have no other visible endometriosis. I began to wonder if endometriosis (both visible or microscopic) could be the cause to tubal ligation pain or other symptoms in many of my patients.
When I find endometriosis, approximately 50% of these patients report no symptoms and the other 50% report symptoms of tubal ligation pain. Mostly they report cramping that increased after their tubal ligation procedure. A few patients report urinary and GI symptoms which began after tubal ligation.
Anatomic Distribution of Pelvic Endometriosis
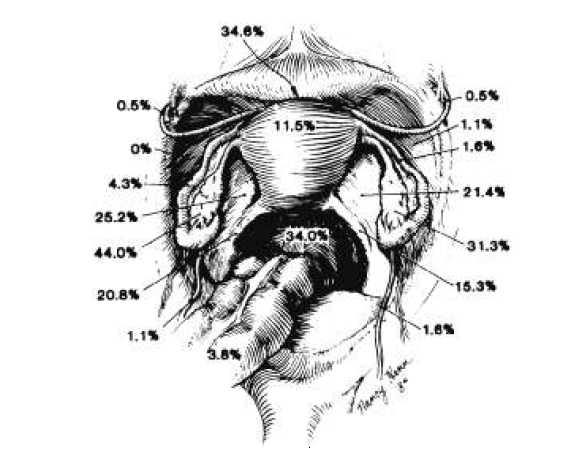
Image adapted from Endometriosis: Pathogenetic Implications of the Anatomic Distribution. S Jenkins, D Olive, A Haney. Obstet Gynecol
A 1986 study by S Jenkins et al demonstrated the locations of visible endometriosis diagnosed by laparoscopy in 186 women who had a preexisting diagnosis of infertility and endometriosis. Most of these patients had not previously undergone tubal sterilization.
This was an important study because it was the first study to evaluate the location of visible endometriosis in a large cohort of women using laparoscopy.
The illustration above nicely demonstrates the typical locations of pelvic endometriosis. The most common locations for visible, pigmented endometriosis were the ovary, broad ligament, the anterior cul de sac , and the posterior cul de sac.
Endometriosis was not commonly observed to involve the fallopian tubes. The overall prevalence of endometriosis involving the fallopian tubes was less than 4%.
Endometriosis as a cause of tubal ligation pain: My observations
Since specializing in tubal reversal and tubal repair surgery I have frequently encountered pigmented visible endometriosis involving the fallopian tubes at the site of tubal ligation and involving the broad ligaments in the immediate area where the tubal ligation was performed. Most of these patients did not report a history of endometriosis and none of these patients had visible endometriosis at the time of their tubal ligation procedures.
 It is important to note my diagnosis of endometriosis is often made on visualization alone. Most commonly we observe superficial pigmented endometriosis and deep nodular pigmented endometriosis. We will also observe non-pigmented endometriosis. It is important to note we may under observe endometriosis because it is either non-pigmented or microscopic. We do not routinely send tissue segments to pathology because of the costs involved during tubal reversal surgery.
It is important to note my diagnosis of endometriosis is often made on visualization alone. Most commonly we observe superficial pigmented endometriosis and deep nodular pigmented endometriosis. We will also observe non-pigmented endometriosis. It is important to note we may under observe endometriosis because it is either non-pigmented or microscopic. We do not routinely send tissue segments to pathology because of the costs involved during tubal reversal surgery.
We do see a variation in the tubal segments in which the segments are visually normal but the tubal muscularis is hypertrophied and fibrotic. It is possible many of these patients have microscopic endometriosis involving the tubal muscularis.
I have collected a series of cases which suggest, for some women, there may be an association between having a tubal ligation and developing endometriosis.
For more information: Can Tubal Ligation Cause Endometriosis?

