







 Almost all types of tubal ligation procedures can be reversed.
Almost all types of tubal ligation procedures can be reversed.
There is only one type that cannot be reversed…only one!
Most types of tubal ligation can be reversed and permanent does not have to be forever.
Women are almost always told by their doctors that tubal ligation is permanent.
They are asked over and over again if they are certain they want their tubes tied.
They are then told over and over again…almost threateningly… they will never have another child and they need to be certain.
Tubal ligation discussions are usually held during or after a difficult pregnancy or while a woman is experiencing a stressful situation. When a woman asks for a tubal ligation they are usually certain they don’t want to ever be pregnant again.
As the future unfolds, many women regret their decision and will only remember the last threatening words of their doctor,
“You know this is permanent, right?”
Almost all types of tubal ligation can be reversed (except for one) but your chance of pregnancy after reversal depends on two factors:
- Type of tubal ligation performed
- Age of the woman at the time of reversal surgery
If you are researching and just want to know more about the types of tubal ligation then this article will give you good overview of the different types currently being performed.
If you want to know what types of tubal ligation procedures can be reversed and what your chances of getting pregnant are then this article is for you!
Types Of Tubal Ligation And Chance Of Reversal Success
Men have it easy. There are very few types of vasectomy.
In fact there is only one main technique for vasectomy with several minor variations. The chance of successful vasectomy reversal depends on one thing….the time that has passed since the vasectomy.
Women on the other hand have it more complicated. There are MANY different types of tubal ligation procedures for women.
The type of tubal ligation your doctor performed depends on how you had your baby (vaginal or c-section) and when after delivery the procedure was done (within 24 hours of birth or weeks or years after giving birth).
The chance of pregnancy depends both on the type of tubal ligation (the least destructive the better) and the age of the woman at the time of reversal (the younger the woman then the more time and ovulations she has after reversal).
Many women mistakenly think the time that has passed since having their tubes tied causes more damage to their tubes. This is not exactly true.
The time that has passed since the tubal ligation is not that important for pregnancy success unless it makes the woman significantly older.
How Do You Figure Out Your Type Of Tubal Ligation?
You can usually figure out your type of tubal ligation by when the procedure was performed.
Tubal ligations are either done close to delivering a baby….or remote from delivering a baby.
Most tubal ligation procedures are done soon after delivery of the last baby. Most of these are cut and tied tubal ligations.
C-sections. During most C-sections the tubes are cut and tied. A few lucky women will have tubal clips placed at the time of C-section. Both can be reversed but reversing tubal clips gives you a higher chance of pregnancy.
Immediately after having a baby. Immediate means within 48 hours of having a vaginal birth and before you are discharged from the hospital. If you have your tubal ligation in the immediate postpartum period (after vaginal birth) then most likely your doctor will make a small incision in your belly button and perform a cut and tied type of tubal ligation. This can also be reversed and the chance of pregnancy will depend on how much tube was actually removed.
Tubal ligations done long after having a baby can be done in several different ways.
Long after having a baby. Long after having a baby usually means 6 weeks or more after having a baby. These are also called interval tubal ligations…or remote from pregnancy. An interval tubal ligation could also be done if you have never been pregnant or never had a baby.
We do not like the term interval….because interval means in between. If you are getting your tubes tied after your last baby…there is no interval..so we prefer to call them tubal ligations done remote after delivery…or remote tubal ligations.
Remote types of tubal ligations are where things can get a little less predictable.
Most remote tubal ligations are laparoscopic tubal ligations (camera inserted through belly button) or hysteroscopic (camera inserted through your vagina and cervix and into your uterus).
- Laparoscopic tubal ligations are usually tubal clips, tubal rings, or tubal burning.
- Hysteroscopic tubal ligations are either Essure coils or Adiana tubal inserts.
All of the above tubal ligations can be revered. Reversing tubal clips and rings gives you the best chance of pregnancy.
Your chances of pregnancy after reversing tubal burning depend on how much tube was burned. You can also get pregnant after reversing Essure and Adiana.
Your chances of pregnancy after reversal or Essure or Adiana depend on the skill of your surgeon and your age.
Your type of tubal ligation can sometimes be determined by when you had the tubal ligation procedure.
The best way to know with 100% certainty your type of tubal ligation is to look at your tubal ligation operative report.
The operative report is a report generated by your doctor after your procedure and it will describe exactly what was done during your procedure. The best place to get a copy of your operative report is from the Medical Records Department where your tubal ligation was performed. Nowadays….your electronic portal may be the best place to get your tubal ligation operative report.
More Information About Operative and Pathology Reports
Ligation and Resection (Tied and Cut): An Overview
Most tubal ligations done during C-sections or soon after a vaginal birth are ligation and resection type tubal ligations…otherwise more commonly known as TIED AND CUT!
Let just put this out in the open…there really is no such thing as tied, cut, AND BURNT. So lets not worry about this…if a doctor tells you they tied, cut, and burned your tubes they are really just trying to convey your tubal ligation is effective and you dont need to worry about a failure.
Ligation and resection is the medical term for ‘tying and cutting’ of the tubes. So if your doctor told you that you were tied and cut then you had a ligation and resection type tubal ligation. Most of these can be reversed as long as only a small amount of tube was removed.
During a ligation and resection type of tubal ligation, the doctor ties a small portion of the tube and then cuts out the tied segment. This usually leaves two healthy segments of tube that can be rejoined during tubal reversal surgery. Tying and cutting of the tubes is only done during C-sections and within the immediate postpartum period.
Tying and cutting of the tubes is easily done during a C-section because the uterus and tubes are easily accessible. After a vaginal birth the doctor will need to make a small incision in your belly button to lift up a small section of your tube to tie and cut.
When a doctor does a tying and cutting procedure…they remove a part of your tube. This is technically a salpingectomy.
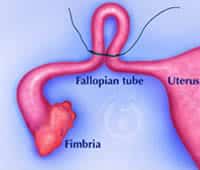
‘Saplingo‘ is a Latin word for tube and ‘-ectomy‘ is a Latin derivative for removal. So salpingectomy means removal of the fallopian tube (either part or whole). They may even throw in the term ‘bilateral‘ and this means both sides.
There are two types of salpingectomy.
Partial salpingectomy. This is the most common type of tying and cutting. During partial salpingectomy they remove a partial part of the tube (4 cm or less). These can usually be reversed.
Total salpingectomy. This type of tying and cutting is becoming more common. During total salpingectomy they remove the total or the ENTIRE fallopian tube on each side. This cannot be reversed.
What you really need to know to determine if your tubes can be reversed is did you have a partial or total salpingectomy…or did they remove a small part (partial) or the entire (total) fallopian tube?
There is only one way you can know for sure and that it to request a copy of your tubal ligation operative report and the pathology report.
Sometimes the operative report will say ‘salpingectomy’ as the method of tubal ligation. It can be a mistake to assume that all of the tube was removed so you really should look at the pathology report. The pathology report is an exact measurement of the amount of tube removed during the tubal ligation.
The fallopian tubes are normally 8 to 10 cm long. Most doctors will remove less than 4 cm.
If your doctor removed 5+ cm or more then it is very likely you had a total salpingectomy. A total salpingectomy is the only tubal ligation that cannot be reversed.
The only type of tubal ligation that cannot be reversed is a complete/total salpingectomy. We cannot reverse…we cannot repair what is not there.
If your operative report says you had a ‘bilateral partial salpingectomy’ then you would be a candidate for tubal reversal.
If your operative report says you had a ‘complete salpingectomy’ or ‘total salpingectomy’ then you would not be a candidate for tubal reversal and you would have to do IVF.
If you are not understanding any of this….then just send us your operative report (and pathology report if available) and we will let you know if you are a candidate for tubal ligation reversal surgery.
Types Of Tying And Cutting Tubal Ligation Procedures
Pomeroy tubal ligation
The most common types of postpartum tubal ligation are the ligation and resection (tying and cutting) procedures:
- Pomeroy tubal ligation procedure
- Parkland tubal ligation procedure
The type of procedure is not so much important as how much of the tube was tied and cut. With both of these the tubes end up looking the same. Both of these tubal ligations methods are easily reversible if they did not remove too much tube.
You can only tell how much tube was removed by comparing the tubal ligation operative report and the pathology report. The pathology report is more accurate.
If they removed less than 3 centimeters then you are good for reversal. If they removed anywhere from 3 to 5 centimeters then reversal is questionable. If they removed more than 5 centimeters then you probably had a complete and total salpingectomy and this cannot be reversed.

Parkland tubal ligation
Pomeroy tubal ligation procedure. The doctor pulls up a loop of your tube, sutures the loop, and cuts the loop part out.
Parkland tubal ligation procedure. The doctor sutures a small section of the tube with one suture on one side and another suture on the other side and cuts out the piece of tube between the suture.
Although the Pomeroy and Parkland tubal ligation procedures are technically different…they both result in a small part of the tube being removed. The health of the tubes is essentially the same after both of these tubal ligation procedures.
These two procedures can easily be reversed and the chance of pregnancy is 60% to 70%.

Irving tubal ligation
Irving tubal ligation procedure. This method involves tying sutures around the fallopian tube and cutting out the segment of tube between the sutures. The ends of the fallopian tubes that come from the uterus are then buried into the uterus in an effort to prevent a tubal ligation failure.
This makes the uterus looks like Mikey Mouse ears!
As long as they removed less than 3 cm then Irving tubal ligation is very reversible and the chance of pregnancy is about 60% to 70%.
Uchida tubal ligation. This method involves cutting the fallopian tube from the overlying connective tissue, placing two sutures, and cutting a segment of the tube out. The end of the tube that comes from the uterus is then ‘hidden’ in the tissue on the side of the uterus.
The Uchida tubal ligation is difficult to understand. If you want to see what this procedure looks like then visit: Illustration of Uchida tubal ligation
Although the Irving and Uchida tubal ligations are not common, we have found that they can be VERY reversible and provide a good chance of pregnancy. This is because they doctors don’t usually remove as much tube with these procedures and the remaining fallopian tube segments are healthy and long.
The chance of pregnancy after reversing a Uchida tubal ligation is about 60% to 70%.
Fimbriectomy tubal ligation. Fimbriectomy tubal ligation used to be a thing of the past…but this older method is becoming more popular.
 This method was usually done by much older doctors in the 1950’s. This is technically a ligation and resection (tying and cutting) type of tubal ligation where the doctor removes the very end of the fallopian tube, which is called the fimbria.
This method was usually done by much older doctors in the 1950’s. This is technically a ligation and resection (tying and cutting) type of tubal ligation where the doctor removes the very end of the fallopian tube, which is called the fimbria.
Fimbriectomy means to remove the fimbria: fimbria (end of tube) + ectomy (to remove).
The fimbria are the very fine finger-like projections at the very end of the tube. These fingers sweep the ovary and guide the egg into the opening of the tube. During a fimbriectomy the doctor removes the very end of each fallopian tube. This causes the remaining tube to heal closed. The egg cannot get into the tube and the sperm cannot get escape to find and fertilize an egg.
Fimbriectomy is becoming more and more popular since 2012.
Some scientist believe the fimbrial cells are where ovarian cancer may be coming from. Some doctors believe that if you remove the end of each tube during a tubal ligation or remove the entire fallopian tube (total salpingectomy) then you MAY decrease the risk of ovarian cancer in the future.
Currently this is not a sure thing and many women are having the ends of their tubes removed at the time of tubal ligation so we can experiment and see if there is a decrease in ovarian cancer in the next 30 years.
Fimbriectomy tubal ligation can also be reversed but the chance of pregnancy is lower with reversal of this type of tubal ligation.
If less than 3 cm of the ends of the tube were removed the chance of pregnancy after reversal of fimbriecotmy tubal ligation ranges from 15% to 40%.
Tying And Cutting Tubal Ligation: Take Home Message
The take home message is that all of the above procedures of tying and cutting are usually reversible as long as they did not remove the entire fallopian tube.
The METHOD is not as important as HOW MUCH TUBE was removed. You can only tell that from looking at the pathology report. In general about 2 out of every 3 patients who get reversal of tied and cut will become pregnant.
You just need to make sure your doctor was not tying and cutting out the entire fallopian tube on each side…this would be a complete salpingectomy. This would not be surgically reversible.
Burning Tubal Ligation Procedures: An Overview
Burning tubal ligation is when the doctor burns a small portion of the fallopian tube. This is usually done remote from pregnancy and laparoscopically with a camera inserted through the belly button.
The medical term for burning is ‘coagulation’ or ‘cautery’. Your doctor will never put on your operative note that your tubes were ‘burned’. Instead they will call it ‘bilateral coagulation’…or burning of both sides.
Most people are not aware but the burning methods are also reversible…and just like cutting and tying it really depends on how much tube the doctors burned. Did they burn a little or a lot?
There are really only two types of burning procedures: bipolar (more common) and monopolar (less common).
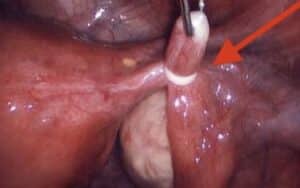
Bipolar coagulation. Bipolar is more of a controlled burning procedure. The doctor grabs the tube with a small tweezer and electric current is passed from one prong of the tweezer to the other prong.

The red circle around the white area shows the burned portion of the Fallopian tube
As long as they did not burn too much then this method can be reversed. Most doctors do a 3-point burn in the middle of the tube. This is usually reversible. If they burned the entire tube then this may not be reversible.
In general the chance of pregnancy after reversal of bipolar coagulation is approximately 50% to 70%.
Monopolar coagulation. Monopolar coagulation is far less common but more of a destructive type of burning. The doctor places a small electric wand type of device and electricity can pass up and down the tube and can damage larger portions of the tube than compared to bipolar coagulation.
Monopolar coagulation can usually be reversed and the chances of pregnancy are usually 50% to 60%.
Burning Tubal Ligation: Take Home Message
Most burned tubal ligations can be reversed and give you a good chance of pregnancy.
The problem with the burning procedures is not the procedures but the doctors…each doctor does the procedure differently. Some doctors burn a little and some burn a lot. Every doctor performs the burning procedure differently.
If you are considering reversal of a burned tubal ligation then it would be a great idea to get a copy of your tubal ligation operative report so we can see how much of each tube was burned.
You will NOT have a pathology report with a tubal burning procedure because no tube is usually removed during this type of procedure.
Tubal Clips: Excellent Method For Reversing
Fallopian tube clips are usually placed during a laparoscopic procedure but occasionally clips can be put on your tubes during a c-section.
 There are two type of tubal clips: Filshie clips and Hulka clips.
There are two type of tubal clips: Filshie clips and Hulka clips.
The Filshie clips are titanium clips. These clips easily show up on x-rays and sometimes on ultrasound.
Hulka clips are plastic clips and are much harder to see on x-ray and ultrasound.
Clips are usually placed across the fallopian tubes during a laparoscopic procedure. One clip is used for each tube. The clips only damage a very small portion of each tube.
The tubal clips cause severe pressure on the tissue underneath the clip. This pressure causes that small portion of the tube to lose blood supply. This tissue dies and get absorbed by the body. The tubal ends soon heal closed and pull apart. The tubal clips are not serving any function after the tube heals closed.
The remaining tubal lengths are usually long and healthy after a tubal clip tubal ligation.
Either of these two types of tubal clips are great for reversing and the chance of pregnancy could be 80% to 90%.
Tubal ring: Great Method For Reversing
Fallopian tube rings are only placed during laparoscopic procedures. These procedures are done well after pregnancy…or at any time if you have never been pregnant.
 During this tubal ligation method a small rubber ring is placed around a small section of the middle of each tube. Tubal rings cannot be seen on x-ray or ultrasound.
During this tubal ligation method a small rubber ring is placed around a small section of the middle of each tube. Tubal rings cannot be seen on x-ray or ultrasound.
Just like the tubal clips, tubal rings cause severe pressure on the tissue trapped inside the ring. This pressure causes the small trapped tissue to lose blood supply. This tissue dies and gets absorbed by the body. The tubal ends soon heal closed and pull apart. The tubal ring is not serving any function after the tube heals closed. The remaining tubal lengths are usually long and healthy after a tubal clip tubal ligation.
Tubal rings…just like tubal clips… are an excellent type of tubal ligation to reverse because the ring does not damage that much tube. Since the tubal rings are a standard size the condition of the tube at the time of the reversal is usually pretty good. The fallopian tube is healthier and usually longer after reversal of tubal rings.
The chance of pregnancy after reversal of a tubal ring type tubal ligation is about 80% to 90%.
Essure Hysteroscopic Tubal Ligation
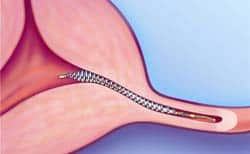
Essure tubal ligation is the newest method of tubal ligation and was introduced in the United States in the early 2000’s. Essure devices consist of two metal coils. The inner coil is a stainless steel coil and the outer coil is a nickel coil. The Essure devices can easily be seen on x-ray. They can be seen with ultrasound but not always with certainty.
 Essure is not really a ‘ligation method’. Ligation means to tie…and there is no tying during an Essure procedure.
Essure is not really a ‘ligation method’. Ligation means to tie…and there is no tying during an Essure procedure.
Rather the Essure coils are inserted into the fallopian tube during a hysteroscopic procedure (camera inserted through the vagina and cervix). The Essure devices are inserted into the very opening of each tube and are allowed to remain in the tube. The devices cause scar tissue to grow through the devices and cause the tubes to be blocked … or occluded.
Technically Essure is a tubal occlusion type of tubal ligation…or devices that cause tubal blockage.
After insertion, scar tissue forms around the coils, blocking off the fallopian tubes and preventing sperm from reaching the egg.
Essure was removed from the US market in 2019 due to impending litigation and the concern for lawsuits from Essure device failures and complaints of chronic pain after device insertion.
Adiana Hysteroscopic Tubal Ligation
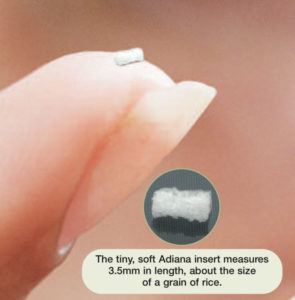
Adiana tubal ligation is very similar to Essure. The Adiana device are small silicone devices (ie plugs) that are inserted into the very opening of the fallopian tubes.
Technically, Adiana is not a tubal ligation but a tubal occlusion (causes closure of the fallopian tube). The Adiana devices cannot be seen with either x-ray or ultrasound. They are so small as to be almost invisible to the naked eye.
 Adiana, like Essure, is one of the newer modern methods of tubal ligation that was introduced to the United States in the early 2000’s. The Adiana method causes the the fallopian tubes to heal closed in the area where the Adiana devices are inserted. The devices are inserted using a hysteroscope (camera place through the vagina and cervix).
Adiana, like Essure, is one of the newer modern methods of tubal ligation that was introduced to the United States in the early 2000’s. The Adiana method causes the the fallopian tubes to heal closed in the area where the Adiana devices are inserted. The devices are inserted using a hysteroscope (camera place through the vagina and cervix).
During the procedure, the doctor inserts the devices and use a microwave energy source to cause damage in the area where the silicone plugs are inserted. After the procedure, scar tissue forms around the silicone inserts, blocking off the fallopian tubes and preventing sperm from reaching the egg.
Adiana was removed from the US market in 2012 when the company was alleged to have inappropriately adopted the patented Essure approach to hysteroscopic tubal occlusion.
Understanding The Types Of Tubal Ligation
If you are looking for greater knowledge then this article should have provided you with a basic review of all the different types of female tubal ligation procedures.
More information: Chances of pregnancy after reversal of all types of tubal ligation with Dr Monteith of A Personal Choice Raleigh North Carolina
 If you want to become pregnant after your tubal ligation then this article should have provide you with the hope most tubal ligations can be reversed.
If you want to become pregnant after your tubal ligation then this article should have provide you with the hope most tubal ligations can be reversed.
You can have another chance to become naturally pregnant again.
Tubal reversal can provide an affordable alternative to in-vitro fertilization (IVF).
If tubal reversal is successful then you have a chance to become pregnant every month and more than once. If you are interested in tubal reversal surgery then you should only trust an expert with your reversal surgery because you may only have one good chance to get it right.
Dr. Monteith exclusively specializes in tubal reversal surgery.
He is the Medical Director of A Personal Choice Tubal Reversal Center in Raleigh, North Carolina. If you would like to know if you are a candidate for reversal center then you should send him a copy of your tubal ligation operative and pathology reports (if available) for a free review.
For more information on how to send your records list: Sending records to Dr Monteith for a free review

