







Tubal ligation reversal involves microsurgical techniques to open and reconnect the fallopian tube segments that remain after a tubal ligation procedure. Usually there are two remaining fallopian tube segments – the proximal tubal segment that emerges from the uterus and the distal tubal segment that ends with the fimbria next to the ovary.
The procedure that connects these separated parts of the fallopian tube is called microsurgical tubotubal anastomosis, or tubal anastomosis for short. Often many refer to the tubal anastomosis procedure as “tubal reversal”.
We specialize in all of these procedures. We perform these procedures as outpatient surgery, at an affordable price, and provide our patients with the ability to become pregnant naturally and more than once. All of these procedures can provide an alternative to in-vitro fertilization.
Tubal ligation reversal: Microsurgical tubal anastomosis
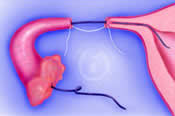
After opening the blocked ends of the tubal segments, a narrow flexible stent is gently threaded through the fallopian tube segments and into the uterine cavity. This ensures the fallopian tube is open from the uterine cavity to the fimbrial end. The newly created tubal openings are then drawn next to each other by placing a suture underneath the fallopian tube segments. The retention suture keeps the tubal edges together, decreases tension, and avoids the likelihood of the tubal segments subsequently pulling apart.
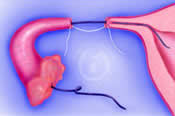
Very fine, permanent microsurgical sutures are used to precisely align the muscular portion (muscularis) and outer layer (serosa), while avoiding the inner layer (mucosa), of the fallopian tube. The tubal stent is then gently withdrawn from the fimbrial end of the tube.
The use of permanent non-absorbable sutures is very important because it allows the tubal edges to heal together and avoids tubal scarring which may occur when temporary non-absorbable sutures are used.
The chance of pregnancy after tubal reversal can be as high as 80%.
Microsurgical salpingostomy for fimbriectomy reversal


Fimbriectomy is an rare type of tubal ligation and differs from other methods of tubal ligation.
Fimbriectomy tubal ligation is performed by removing the very end of the tube (the fimbrial end next to the ovary) leaving behind one tubal segment attached to the uterus. After fimbriectomy, the remaining tubal segment can be opened by the technique of microsurgical salpingostomy.
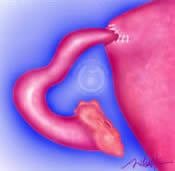
Microsurgical salpingostomy is performed by creating a small opening in the remaining end of the fallopian tube with a microsurgical needle electrode. The newly created opening is then enlarged and gently folded back like the petals of a flower to allow the internal endothelial lining to emerge and extend over the opened tubal end.
Since healthy tubal endothelium is covered with cilia – the hairline projections that beat in coordinated waves – the new tubal opening or ostium can capture an egg as it is released from the ovary and propel it into the tube just as the fimbrial end of the tube does normally. Fine sutures are carefully placed around the circumference of the folded back end of the fallopian tube to prevent scar formation and closure.
The chance of pregnancy after fimbriectomy reversal range from 15% to 40% and depends on the health and length of the remaining fallopian tube.
Microsurgical tubal implantation
In some cases, a tubal ligation procedure leaves only the distal portion of the fallopian tube and no proximal tubal opening into the uterus.
In this situation, a new opening can be created through the uterine muscle and the remaining tubal segment inserted into the uterine cavity.
This microsurgical procedure is called tubal implantation, tubouterine implantation, or uterotubal implantation.
The chance of pregnancy after tubal implantation at our center ranges from 30% to 50%.

