







I recently received an email from a patient who had an ectopic pregnancy subsequent to her tubal reversal. Unfortunately, the pregnancy continued to the point of tubal rupture with the loss of the fallopian tube.
Patient’s History
I was hoping you could help me understand why my ectopic pregnancy was not detected early enough to prevent the loss of my right tube. I need to know this for the future as after my surgery I have only my left tube remaining.
I went to my doctor at approximately 3 weeks pregnant and made sure that they understood the importance of checking for ectopic pregnancy. I gave them a copy of your instructions and told them my goal is to prevent losing my tube if it is ectopic, so I told them to please check and make sure it is not ectopic. They did blood work 3 times and did a vaginal ultrasound at approximately 4 weeks and said everything was normal and the sac was in the uterus, not the tube. They did not check anything again until I spotted Tuesday of this week. I went in Wednesday and they did a vaginal ultrasound and said it was ectopic with a heartbeat and I needed surgery and my tube would have to be removed.
My tube was removed because it was starting to rupture. I never expected that to happen because I took the precautions necessary.
Can you please tell me what normal pregnancy hormone levels are for each week of pregnancy versus ectopic hormone levels?
When is an ectopic visible on ultrasound? Could this have been prevented? Was there anything else that could have been done?
Role of Serum HCG in Early Pregnancy Monitoring
HCG levels alone do not differentiate between uterine and ectopic pregnancy. The HCG levels provide the earliest evidence of whether implantation has occurred successfully (but not where it has occurred) and indicate when ultrasound examination should be able to find a gestation sac if the pregnancy is in the uterine cavity. This occurs when serum HCG reaches 1500-2000 mIU/dL. If serum HCG levels are rising too slowly, or if ultrasound does not find a gestation sac in the uterus when HCG is at the level of 1500-2000, then the pregnancy is not a normal one. It could be outside of the uterus (ectopic) or it could be an abnormal pregnancy in the uterus (blighted ovum).
Role of Transvaginal Ultrasound
A careful transvaginal ultrasound exam can detect a normally developing pregnancy in the uterus very early. It is apparent in this case that the initial ultrasound findings were not interpreted correctly. How could this occur?
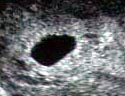 An intrauterine gestation sac is a dark oval shaped area of fluid surrounded by a bright white ring or halo (the trophoblastic tissue). Probably in this case there was a small amount of fluid in the uterine cavity that was mistakenly thought to be a gestation sac. This has been described as a “pseudo-sac”. A pseudo-sac does not have the distinct white halo or ring of a true gestation sac.
An intrauterine gestation sac is a dark oval shaped area of fluid surrounded by a bright white ring or halo (the trophoblastic tissue). Probably in this case there was a small amount of fluid in the uterine cavity that was mistakenly thought to be a gestation sac. This has been described as a “pseudo-sac”. A pseudo-sac does not have the distinct white halo or ring of a true gestation sac.
In a normally developing uterine pregnancy, a follow-up ultrasound exam will show the presence of a yolk sac (the small circle within the gestation sac) within a week of the appearance of the gestation sac. If the initial ultrasound exam had been followed-up with another ultrasound scan, it would have shown that this was not a normal uterine pregnancy.
Comment
There is an increased risk of ectopic pregnancy following tubal reversal surgery. Our follow-up pregnancy statistics show that the risk of ectopic pregnancy remains constant with each pregnancy. In other words, it is the same for a first, second, third, or subsequent pregnancy after tubal reversal surgery. It is important, therefore, to monitor any pregnancy after tubal reversal early and closely.
Recommendations for early pregnancy monitoring are given on our website page entitled I’m Pregnant. Although the recomended tests were performed, the most critical one – the ultrasound exam to document the location of the gestation sac – was interpreted erroneously.
An experienced ultrasonographer should be able to differentiate between a true gestation sac and a pseudo-sac by the presence or absence of the bright halo surrounding the fluid filled sac. If there is any doubt, a repeat ultrasound exam looking for the appearance of a yolk sac should be performed.
Although ectopic pregnancy is not preventable, the complication of tubal rupture always should be. In the absence of clear ultrasound evidence of an intrauterine pregnancy, early treatment with Methotrexate is recommended. It is important to monitor serum HCG levels until the HCG level returns to less than 10 mIU/dL. This will prevent a possible ectopic pregnancy from advancing to the complication of tubal rupture.

